
Why & When Laparoscopic PCOD drilling in Infertility

Video: https://youtu.be/SwVm8aJY9BU
Why:
Laparoscopic drilling is advisable when patient has PCOD and she is trying to conceive with weight reduction & natural conception with or without ovarian induction with Clomipen, Leterazol and follicular study with TVUSG/sonography for at least more than one year without positive result. If her age is less than 30 years, its advisable to try, checking both fallopian tubes laparoscopically during laparoscopic drilling before ovarian induction with gonadotrophins injection with IUI & ART/IVF.
Objective:
Patient present to us with Obesity, hirsutism, irregular/delayed cycles, anovulation & Infertility. TVUSG shows peripherally placed multiple follicles with hyperthicosis of stroma & large ovaries. PCOD drilling is indicated in Clomiphen resistant PCOD, where weight reduction & metformin had been tried sufficiently (for six months) in the past. In the past, wedge resection by Laparotomy was routine practice for fertility enhancement. Today laparoscopic PCOD drilling has become very popular fertility enhancing surgery. As compared to Gonadotrophin (pure FSH) injections i.e. ART with super ovulation, PCOD drilling had following advantages after surgery: 60-70% Ovulation rate, 40-50% Pregnancy rate, reduced abortion & OHSS following drilling, reduced requirement of CC.HMG/FSH/hCG following drilling. Effect of drilling lasts for nine months. According to the size of ovary 4 to 12 punctures should be made on both ovaries.
Benefits of Laparoscopy Surgery:
- Shorter Hospital stay.
- Earlier return to your routine work.
- Cosmetically vary small scar.
- Less pain after operation.
- Best fertility enhancement & Fertility results following Laparoscopy.
- Video-live operative file available in CD/DVD for future reference (Transparency about surgical procedure).
- The possibility of post-operative adhesion formation will be less, and the possibility of pain because of post-operative adhesions will also be less.
Pre-operative Check Lists :
- Pre-operative Lab. Investigation for Surgery (Urine complete & Blood complete, HbsAg, HIV, HCV, R.B.S. etc.); Pelvic Trance vaginal USG report.
- Specific Investigations for Infertility (Blood reports: – Endocrine-S.FSH, S. LH, S.TSH, S.PRL, S.AMH, Genetic, Husband’s Semen report etc.)
- Pre-operative physician fitness with ECG.
- Operation planned from 4th to 10th day of Menstrual Cycle
- Enema & preparation/shaving of local parts.
No. Of Cuts on Abdomen:
Three cuts: One of 5 mm and second & third of 3 mm size.
Average Stay in Hospital:
4 to 6 hours. (DAY CARE SURGERY)
Average Duration of Surgery:
10 to 20 minutes
Average Blood loss during Surgery:
10-30 cc.
Average time after operation to resume normal activities/work:
Within 24 hours.
Anesthesia:
General Anesthesia (Patient will not feel any pain in Operation Theatre during surgery)
Operative Procedure:
Inside the Umbilicus small needle is introduced and Co2 gas is insufflated inside abdomen. Rather than creating a large incision and opening up the body, tiny incisions are made and a laparoscope is inserted. This slim scope has a lighted end. It takes pictures – actually fiber optic images – and sends them to a monitor so the surgeon can see what is going on inside.
Performing Laparoscopy usually only requires three tiny incisions less than one half inch, (about 5-10 millimeters) in length. One incision is made inside the navel, and another two are usually made near the bikini line. The first incision allows a needle to be injected into the abdomen so carbon dioxide gas can be pumped inside the cavity of the abdomen, which helps to keep intestines & omentum up and away from organs. This allows the surgeon a better view and more working space to maneuver the laparoscope and surgical tools as needed.
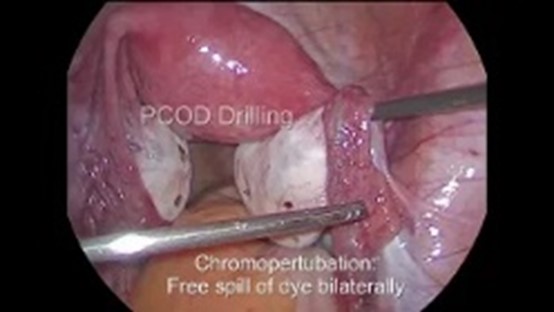
Cystic Ovary is lifted with suction irrigation cannula from one port and High frequency needle is used to puncture the ovarian surface perpendicularly from opposite side port. No. Of punctures are decided on the based of severity of PCOD & of the size of enlarged ovaries. Haemostasis is checked & Ringer lactate poured over ovaries after Drilling.
Post-operative Course:
Patient remains drowsy/sedated for 2-3 hours after laparoscopy but conscious & pain free. Patient can take fluids 3-4 hours after laparoscopy & light food after 4-6 hours. She may feel little abdominal pain after laparoscopy for 24 hours but it can be relived with pain killer tabs. Most of the patients can walk normally without support and can take normal diet 6-8 hours after the laparoscopy. She can be discharged on the same day of the operation. Few patients may feel nausea & vomiting after laparoscopy, which can be very well controlled with injection in post-operative room. Patient can do her normal activity within 24 hours after laparoscopy. Patient is advised to take antibiotics & analgesic tabs. for 5 days following laparoscopy. Patient is advised to report to doctor for severe pain or bleeding or fever in postoperative period (Day-1 to Day-5) immediately. Patient is advised to come for follow up 7 days after the Laparoscopy.
